

The acromioclavicular (AC) joint is the only direct link between the scapula (shoulder blade) and the rest of the skeleton. It is a relatively small joint, but at the same time serves as the skeletal support for the entire upper extremity.
Therefore it is exposed to a great deal of force, especially during traumatic injuries. Typically the AC joint is compressed and sheared when the top of the shoulder blade strikes a blunt object with a great deal of force, such as a high-energy tackle in football or a bicycle crash directly onto the shoulder.
AC joint injuries are classified by the amount of collateral damage to the surrounding ligaments and by the amount of displacement (movement) of the clavicle relative to the acromion. Type I and II injuries are just sprains—the stabilizing ligaments are stretched but not entirely torn, so the clavicle and acromion maintain their normal relationship.
In Type III injuries, the coraco-clavicular ligaments tear, disrupting the last soft-tissue connection between the clavicle and the acromion. The scapula and entire upper extremity tend to sag down with gravity, while the various muscle attachments to the clavicle tend to pull it up (toward the head).
Type IV and V injuries are essentially Type III injuries where the clavicle has been pushed through some of that surrounding muscle, causing it to get stuck far out of position. Type VI injuries are
Dr. Rahul Bade is a specialist Knee & Shoulder Surgeon.
Treatment for AC joint injuries has evolved significantly over the past two decades. As before, Type I and II injuries are best treated without surgery. A sling is used early-on for comfort, and the shoulder is mobilized early and often to prevent stiffness. Pain typically subsides after a few weeks. Physical therapy can be helpful if stiffness or weakness are a problem.
Type IV and V injuries are typically treated surgically. These injuries cause a fair amount of dysfunction, even after the initial trauma heals, because the clavicle is stuck out of place. Surgery is best done in the first few weeks after the initial injury, because the clavicle can be difficult to position back into place once it settles into its new position. Also, you can take advantage of freshly healing ligaments if the injury is addressed in a reasonable amount of time.
Type III injuries are controversial. There is good evidence to show that, for most patients, type III injuries can result in a normally functioning shoulder if they are left alone, although the appearance will change somewhat because of the prominent clavicle “bump.” Some patients (somewhere between 20-40%) will develop chronic pain in the AC joint, or will develop such an unstable joint that the shoulder is not usable (for instance, significant painful popping/subluxation of the clavicle when the arm is lifted above shoulder level). For these patients, late surgery is a good option. There is good evidence to show that patients with Type III injuries who opt for late surgery have just as good an outcome as patients who have immediate surgery. For some elite level athletes, early surgery can make sense depending on the timing of their training or competition season, so they can avoid the potential of having to miss training or competition later.
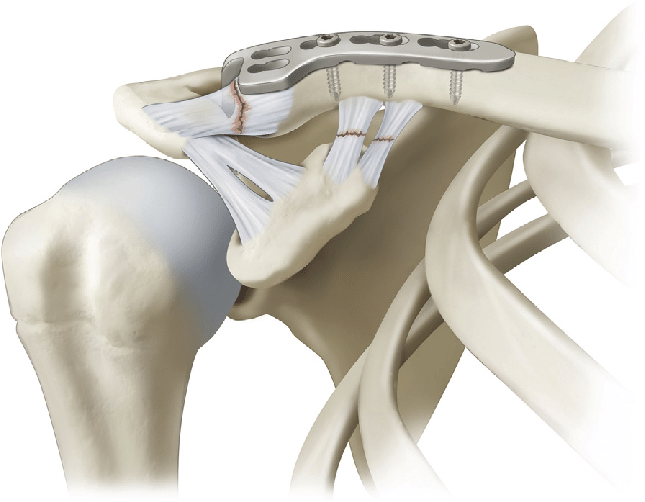
Many operations have been described to address AC joint injuries. Over the past few years, techniques have evolved significantly. The surgery can now often be done arthroscopically. This reduces the dissection that is needed in front of clavicle, reducing damage to surrounding muscles during the procedure. At MOI, a “belt and suspenders” approach is used, adding both mechanical and biological fixation to hold the clavicle in place. This results in extremely sturdy fixation, while providing biologic tissue that can heal into permanent collagen support.
Copyright © 2025 Dr. Rahul Bade | All Rights Reserved | Created & Crafted by Itorix Infotech LLP
Need to bounce off ideas for an upcoming project or digital campaign? Looking to transform your business with the implementation of full potential digital marketing?
For any career inquiries, please visit our careers page here.
