

An all-arthroscopic rotator cuff repair is a challenging procedure that can be successfully performed for treatment of supraspinatus and infraspinatus tendon tears. Often, tears of the subscapularis tendon do not involve the entire tendon, and retraction of the torn edge is within 1 to 2 cm of its attachment site. Occasionally, the entire tendon is torn and retracted medially to the glenoid. This article outlines the examination, preoperative planning, complications, and details the steps necessary to perform this procedure on all types of subscapularis tears.
Rotator cuff tears represent one of the most common reasons for shoulder pain. The rotator cuff is a group of muscles and tendons very important for the function of the shoulder joint. Do you know why the name “cuff” is used? This is because the tendons of these four muscles blend together as they attach to the arm bone (humerus). The subscapularis comes from the undersurface of the shoulder blade and attaches to a flat surface in the front of the humerus, called the lesser tuberosity. The supraspinatus, infraspinatus and teres minor come from the back and side of the shoulder blade, attaching to a larger platform of bone, the greater tuberosity. The biceps tendon in the front of the arm has two tendon ends towards the shoulder; one of them (the tendon of the long head of the biceps) lies in parallel to the upper portion of the subscapularis tendon and the front portion of the supraspinatus tendon, in the so-called interval region. Although the rotator cuff can get injured at the muscle-tendon junction, most commonly a rotator cuff tear involves tendon fiber detachment off of bone. These tears may be the result of an injury (you can read our post on acute rotator cuff tears) or wear and degeneration (read our post on chronic rotator cuff tears).
Individuals with rotator cuff tears often feel a combination of pain and weakness. Over time, their shoulder may become stiff as well. Most people feel a dull, deep ache on the side of the shoulder. It is especially painful when trying to reach up or out, or with sudden motion of the shoulder. Pain is particularly bothersome at night. Weakness varies: individuals with smaller tears may have near normal strength, whereas very large tears, involving most of the cuff, may make it impossible to raise the arm. Not uncommonly, individuals with a torn rotator cuff realize that it is easier to raise the affected arm with the assistance of their other hand, or by keeping the elbow bent. Bringing the arm down from an upward position becomes particularly painful. Medical attention should definitely be sought soon when an individual suddenly looses the ability to raise the arm after a shoulder injury; however, most cuff tears develop slowly over time. Shoulder specialists evaluate patients suspected of having a cuff tear by assessing motion and strength. There are a few ways to test for shoulder strength that are particularly useful. In the subscapularis bear hug test, the patient is requested to place the flat palm of the hand on the opposite shoulder with the elbow up, and the doctor tries to lift the arm off the shoulder. In the supraspinatus empty can test, the patient is asked to extend their arms forward, with the thumb pointing down, as the doctor tries to push the arm down. Testing the strength of the patient’s ability to push out with their arm at their side will test the integrity of the infraspinatus and teres minor.
This surgical procedure is almost always performed under general anesthesia. Some times, your anesthesiologist will recommend an injection of a local anesthetic in your neck area, into the bundle of nerves that supply sensation to the arm, the brachial plexus. Blocking the brachial plexus temporarily with local anesthesia decreases or completely eliminates shoulder pain for a number of hours after surgery.
The bed where you will lay in the operating room is articulated, which will allow the surgeon to position you on your side or in a sitting up position for easy access to the shoulder. A mechanical device is often used to hold the arm in different positions. The shoulder is isolated from the rest of the body with drapes to avoid infection.
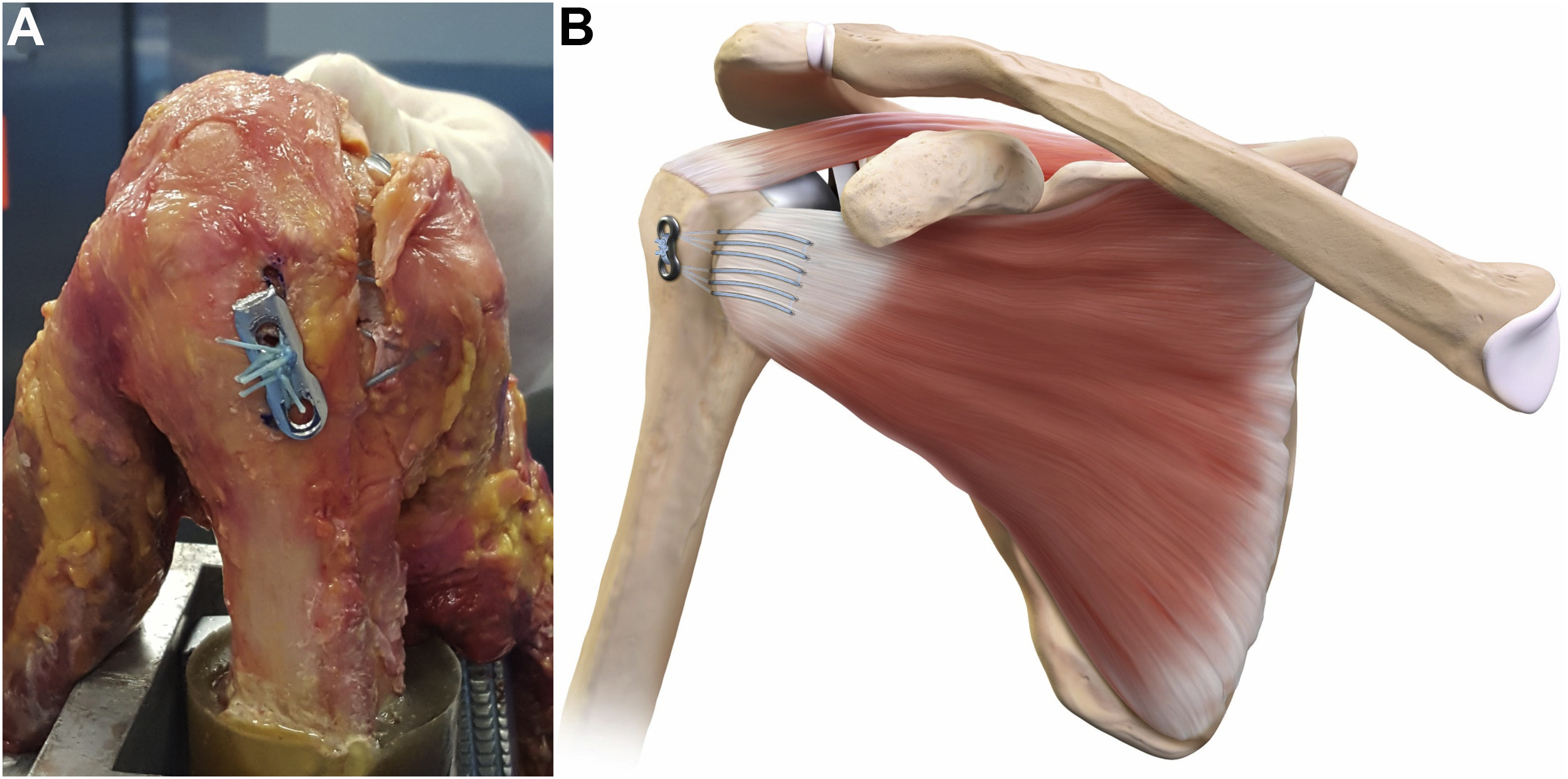
A camera is introduced into the shoulder using a metal sleeve -called a cannula- through a small skin cut. Additional small skin cuts are used as needed to introduce additional instruments. Once the scar tissue and the so-called bursa are removed, the bony surface that will receive the tendon end is prepared by cleaning all scar tissue and lightly brushing the bone with a burr. Bone preparation facilitates tendon to bone healing. Anchors are the most common devices used for cuff tendon reattachment to bone. These anchors come loaded with sutures or tapes. They are screwed or tapped into the bone to gain strong purchase. Therefore, the sutures or tapes are secured to bone and can be weaved through the tendons, and are either tied or secured to additional anchors. The tendon edge is thus compressed to the bone and hopefully healing occurs. Remember how the biceps tendon lies in the interval region? In some individuals with cuff tearing, the long head of the biceps is either partially torn or very loose and unstable. In these circumstances, the long head of the biceps is addressed as well by releasing it, lengthening it, or fixing the biceps tendon in a new spot (this part of the procedure is called biceps tenodesis).
Copyright © 2023 Dr. Rahul Bade | All Rights Reserved | Created & Crafted by Itorix Infotech LLP
Need to bounce off ideas for an upcoming project or digital campaign? Looking to transform your business with the implementation of full potential digital marketing?
For any career inquiries, please visit our careers page here.