

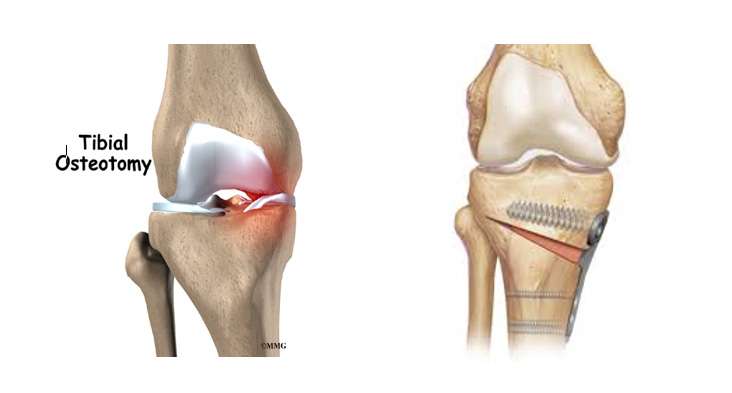
A high tibial osteotomy is a surgical procedure that realigns the knee joint by correcting the deformity in the proximal tibia in partial knee arthritis.
If you are suffering from severe pain either on medial (inner) or lateral (outer) side of your knee limiting your activities you might be suffering from partial knee arthritis (one compartment). When the severe arthritis is limited to one compartment, high tibial osteotomy is also a good option
Your knee joint is divided into three compartments, medial compartment (the inside part of the knee), lateral compartment (the outside part) and patellofemoral compartment (the front of the knee between the kneecap and thighbone)
This surgery can delay or prevent the need for a partial or total knee replacement by preserving damaged joint tissue. There are no restrictions on physical activities. You can resume all normal activities
By shifting the body weight from the damaged side of the joint to the normal side, an osteotomy can relieve pain and significantly improve function in an arthritic knee
Copyright © 2023 Dr. Rahul Bade | All Rights Reserved | Created & Crafted by Itorix Infotech LLP
Need to bounce off ideas for an upcoming project or digital campaign? Looking to transform your business with the implementation of full potential digital marketing?
For any career inquiries, please visit our careers page here.